Concerns Persist Over Involuntary Treatment of Individuals in Psychiatric Hospitals, Ombudsman States
Concerns persist regarding the involuntary treatment of individuals in psychiatric hospitals, an issue that has become chronic. This statement was released by the Ombudsman’s Office.
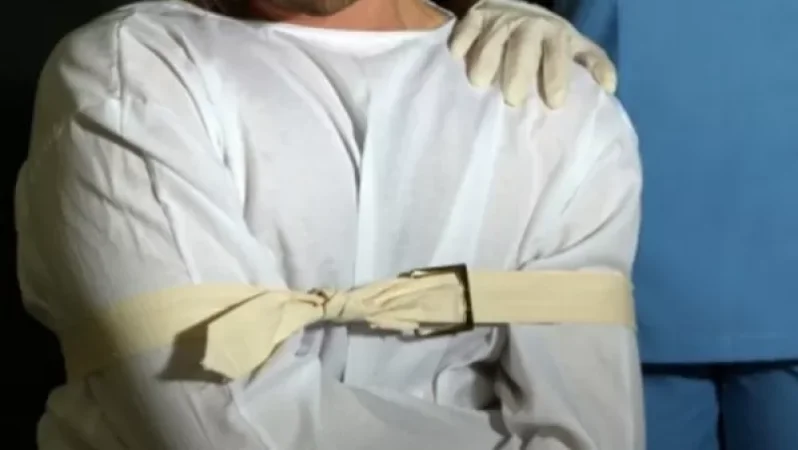
The consent for psychiatric treatment is often formal, and individuals in psychiatric facilities are deprived of their freedom, experiencing gross violations of their rights.
Judicial decisions are formal and superficial, lacking sufficient grounds and typically relying on template formulations without offering any guarantees for the individual.
For instance, a visit to the Armash Health Center last year revealed that management had submitted a petition to the court for involuntary treatment for 19 individuals in two groups, and at the time of the visit, court decisions concerning 7 of these individuals had not yet been issued.
The Ombudsman, in his capacity as the National Preventive Mechanism, examined all documents and noted that the “Medical Commission’s Conclusion” was missing in patient records or related entries were absent in the periods before or after the evaluation by the medical commission.
In some cases, the results of the commission’s conclusion were added to patient records as an additional page, despite the original number of pages not being exhausted.
There were also no entries about the refusal of treatment or hospitalization for individuals with mental health issues. Medical examinations and corresponding notes continued to be made in the accepted “format” monthly, and did not reflect the basis for initiating the involuntary treatment of patients.
Moreover, although the “Medical Commission’s Conclusion” noted that a person with mental health issues “poses a danger in outpatient conditions” or “poses a serious threat to himself and his surroundings due to his mental state,” there were no corroborating records in the medical histories.
Records preceding or following the petition were described without indicating negative dynamics in the patient's mental state, generally portraying a stable or sometimes even positive state.
The petitions submitted to the court for the initiation of involuntary treatment had a typical character, with main formulations repeating, except for the patients' full names and diagnoses.
In all petitions presented to the court, it was noted that “...there is a lack of critical understanding regarding his disease, thereby refusing inpatient treatment, and the failure to undergo treatment may worsen the patient’s mental condition,” “he lacks criticism of his disease, and requires involuntary inpatient treatment and care,” and “we request that this application be accepted for processing and subjected to the law for involuntary hospitalization and treatment in a psychiatric hospital, as he poses a serious threat to himself and his surroundings.”
Neither the petitions nor the medical histories of those with mental health issues typically contained records of the patient’s refusal of hospitalization and treatment. For example, according to a record in the medical history, the patient was admitted to the Armash Health Center for voluntary treatment on May 26, 2020; however, on December 11 of the same year, the center’s management submitted a petition for involuntary treatment, despite ongoing notes in the patient’s history indicating that he was “mainly in a calm state,” “the consciousness is clear,” “he is communicative,” “responds to questions adequately,” “comprehends and maintains hospital order and regulations.”
In these cases, the medical histories do not reflect any legal basis for starting involuntary treatment. These circumstances raise serious concerns about the artificial and baseless nature of the involuntary treatment process.
Instead of properly securing informed consent for hospitalization and treatment, the uniform petitions presented to the court based on such typical “Medical Commission Conclusions,” without proper substantiation of the individual’s risk and necessity for hospitalization, are highly problematic.
It is particularly concerning that over the years, a group of patients who were “voluntary” treated have become inexplicably deemed “highly dangerous to themselves and their surroundings” during the same timeframe, with no substantiation found in the notes made by their treating physicians in their medical histories.
It is gravely alarming that such typical petitions have not raised any doubts among judges who have issued enforcement orders regarding the initiation of involuntary treatment. On the contrary, the judicial decisions have generally been based on the typical formulations presented in the psychiatric organizations’ petitions, without adequate arguments supporting them.
These judicial acts mainly differ only in the names and diagnoses of the patients, which indicates that the enforcement orders regarding involuntary treatment are also of a typical nature.
The Ombudsman reiterates that the need for care for individuals with mental health issues and the lack or absence of relevant social services cannot and should not serve as a basis for initiating involuntary treatment.
Community-based services for individuals with mental health issues, their diversity, and accessibility must be guaranteed by the state. The absence of such services should not justify the ongoing confinement of individuals with mental health issues in psychiatric organizations against their will or the extension of involuntary treatment measures that deprive individuals of their freedom.
Similar issues have also been recorded by the Ombudsman, acting as a preventive mechanism, in other psychiatric establishments.
Նմանատիպ հոդվածներ



Ավելին Society բաժնից

ՏԵՍԱՆՅՈՒԹ․ Արտակարգ դեպք՝ Գյումրիում․ որոշ փողոցներ անանցանելի են դարձել

Ռուսաստանի սանկցիաները շարունակվում են, այլընտրանք չկա․ «Հրապարակ»

Օրենքով գող կկալանավորվի. հայտարարվել է հետախուզում
